- Nigeria’s national census of 2006, counted population of 7.5 million in Onitsha and its surrounding communities.
- Nigeria’s population now stands at 200 million.
- Healthcare expenditures in Nigeria are 3.7% of GDP, compared with the United States’ 11.7%
The latest census of facilities providing primary, secondary and tertiary medical care by the Federal Ministry of Health of Nigeria reveals the following:
| Where | Number of Hospitals and Clinics |
|---|---|
| All of Nigeria | 41,015 |
| Lagos (most populous City) | 2,261 |
| Anambra State | 1,561 |
| Onitsha | 445 |
| Okoti-Odekpe (Ogbaru LGA) | 0 |
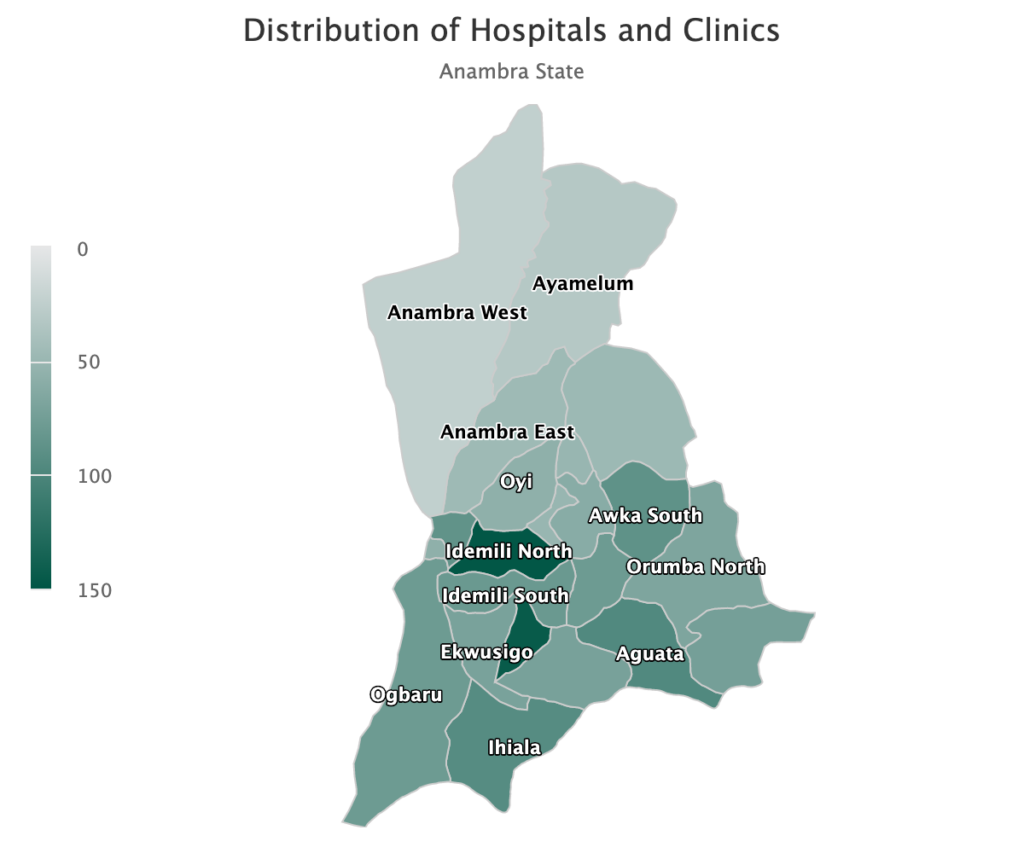
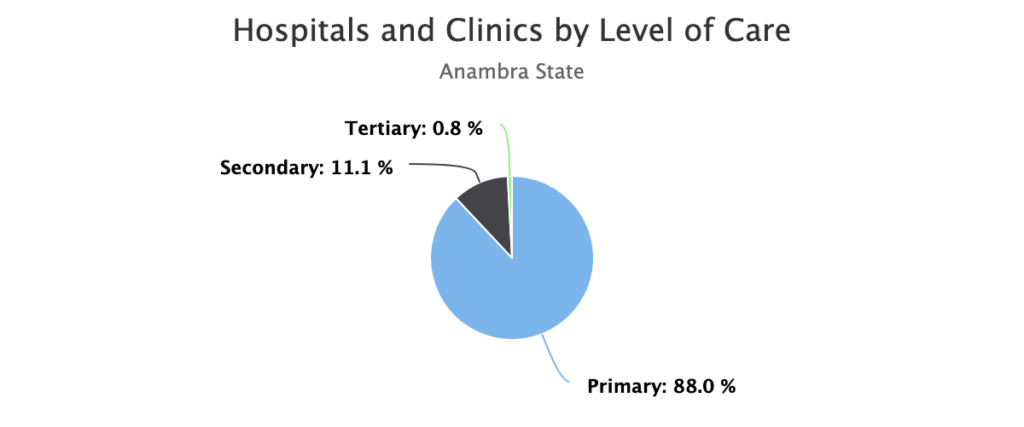
The graphics produced by the Nigeria Health Ministry’s reveal the lack of hospitals to serve the 200 million Nigerian population. They also highlight the few hospitals serving the Southeastern Nigerian State of Anambra, one of the most populous Nigerian states. The hospital will be built in the rural area known as Ogburu Local Government Area (LGA). The Okoti-Odekpe community whose local Chief and residents donated the property for the hospital, is located within Ogburu LGA. These graphics were downloaded on October 25, 2019 from https://health.gov.ng and https://hfr.health.gov.ng.